**Periods! Can’t live with them, can’t do without them!
Poly Cystic Ovarian Syndrome – PCOS

ð affects 10% of women, worldwide,
within their reproductive years (around age 12–45)
> What is PCOS ??
 |
Normal Menstrual Cycle |
Simply put, a hormonal disorder that can cause any number of hair splitting nightmares a woman can possibly think of. From the fat fiasco to acne, oily skin, dandruff, skin discoloration, fits of anger and irritation, sleep apnea (a temporary suspension or obstruction in breathing), mood swings and fatigue, pelvic pain especially during intercourse, abdominal fullness, increased bladder pressure, nausea, breast tenderness to lack of self confidence and depression that stems from all the symptoms not so womanly- Anovulation: failure to ovulate (release of egg from ovaries), Amenorrhea: irregular periods, masculinizing or male-like affects; that includes male pattern hair growth (Hirsutism) and Infertility.
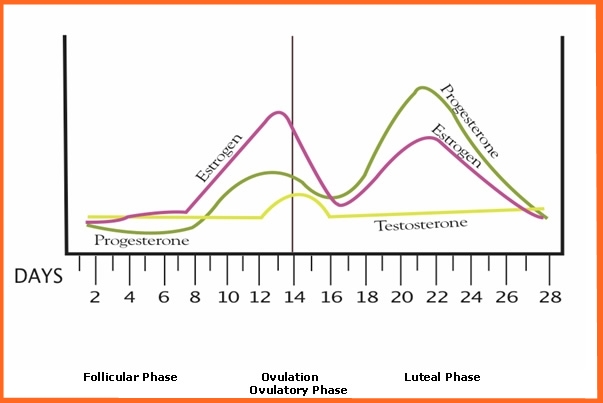 |
Complete Cycle with Testosterone |
Every woman has testosterone, just like every man has female hormones in minute quantities. In fact women have a regular testosterone cycle that occurs synchronously with female hormonal cycles of menses.
Testosterone levels peak at ovulation that increases sexual libido and desire.
Medically PCOS is defined by increased androgen (male hormones such as testosterone) and increased androgen activity beyond the normal range. Although, precise cause of PCOS manifestation remains to be pin-pointed, it is strongly correlated to conditions of Diabetes, Insulin resistance (inability of fat and muscle cells to respond to circulating Insulin, resulting in increased levels of blood sugar; may be genetic) and Obesity.
**PCOS affects WOMEN with FUNCTIONING OVARIES and so misinterpreting this disorder for a supposed male-ing or sex disorder or gender conversion is plain ridiculous
Diagnosis & Prognosis:

Most women are diagnosed with PCOS by a pelvic ultrasound following complaints of irregular periods. Sonograms show a cystic ovary as peripherally ringed by a ‘string of pearls’ (bubbles) of protruding cysts as opposed to a smooth bulb of ovarian tissue. Every normal ovary also has cysts called functional or physiological cysts. These are fluid filled, thin walled sacs that contain the maturing egg, also called follicles. Failure of follicular maturation (arresting egg development) and subsequent release of egg, due to disproportionate hormonal stimulation (varying levels of luteinizing hormone (LH), androgens and circulating Insulin) results in abnormally large fluid filled sacs- diseased cysts that morph into testosterone producing tissue.
How?
In obese individuals, enzyme Aromatase contained in adipose tissue converts androstenedione to estrone and testosterone to estradiol. Bluntly, more the fat, wider the paradox of having both excess androgens (which are responsible for hirsutism and virilization) and estrogens (which inhibits FSH- follicle stimulating hormone via negative feedback). LH proportionately increases triggering ovarian androgen production through cysts.

Also, with Insulin resistance, circulating Insulin levels surge (Hyperinsulinemia) that increases GnRH (Gonadotropin releasing hormone) pulse frequency leading to LH dominance over FSH. Net result is increased ovarian androgen production, decreased follicular maturation, and decreased SHBG (Sex hormone binding globin- a glycoprotein that inhibits hormones testosterone and estradiol) activity; leading to the development of PCOS.

Apart from pelvic ultrasounds, serological assays indicating elevated levels of Insulin, Homocysteine (A homologue of amino acid Cysteine, whose increasing levels increases risks to cardiovascular diseases and is also associated with PCOS) and Androgens (male hormones: Androstenedione, Testosterone and Dehydroepiandrosterone sulfate ) can provide a fail-proof assessment of hormonal imbalance characteristic of PCOS. Ratios of LH:FSH exceeding 1:1 on day 3 of menses and low levels of SHBG are also indicative of PCOS. A typical 2 hour Glucose tolerance test (GTT) may also be conducted to establish Insulin tolerance.
In GTT, patients are instructed to fast for 8-12 hours prior to test (water is allowed). At zero time, blood sample is drawn to determine a baseline or control for subsequent blood sugar estimation. Following, the patient is given, a measured dose of glucose solution to be taken within 5 minutes time frame. Blood is thereafter, drawn at regular intervals for glucose, sometimes Insulin measurement, over a period of 2 hours.
Other assays may be conducted to rule out disorders with symptoms similar to PCOS. These involve Prolactin (for Hyperprolactenemia), TSH-Thyroid stimulating hormone (for hypothyroidism) and 17-hydroxyprogesterone to rule out 21-hydroxylase deficiency (Congenital Adrenal hyperplasia).
 Rarely, a Laparoscopic examination may be carried out to reveal a thickened, smooth, pearl-white ovarian surface indicative of PCOS. However, patients must know that this is NOT required and they can resort to non-invasive diagnostic procedures that are just as effective.
Rarely, a Laparoscopic examination may be carried out to reveal a thickened, smooth, pearl-white ovarian surface indicative of PCOS. However, patients must know that this is NOT required and they can resort to non-invasive diagnostic procedures that are just as effective.Personally one could check for the thickness and lubricity of vaginal discharges. Vaginal fluids change their texture as a function of menses. During ovulation, vaginal discharges are freer flowing and stretchy fluid like, to facilitate sperms to easily swim through incase of copulation, aiding in effective fertilization of the released egg. At other phases of menses, when only estrogen surges, the discharges assume a thicker form. And thus, presence of a continuous, creamy or egg-white vaginal discharge throughout a month or more is a definite indication of hormonal imbalance.
Finally, effective diagnosis is much a matter of broad minded attitude than the mere act of seeking medical intervention. Your clinician should be made aware of your menstrual and sexual history. Specifically menstrual patterns, episodes of weight gain, excessive hair growth, vaginal discharges and unusual breast development, both retarded and proliferative growth must be reported. Remember questions that are most sensitive are also most likely to be specific and crucial to diagnosis.
Ladies > Do NOT let petty things like shame, pride or other irrelevant crap come in the way of an effective diagnosis and treatment. Your health and well-being is your responsibility. A thorough physical examination including breasts, pubic hair and the vaginal area is crucial to assess the extent of PCOS manifestation. The general physician usually refers a PCOS suspected patient to a gynecologist, who in turn undertakes physical examination and prescribes the necessary diagnostic tests. Ultimately the treatment is supervised by a certified endocrinologist. It is always better, that PCOS is detected as early as possible to prevent the umpteen numbers of other risks that will follow.
These include:
- Endometrial hyperplasia- Uterine lining over-accumulates under prolonged stimulation of estrogen with the lack of progesterone, during absence of subsequent menses leading to endometrial cancer
- Insulin resistance/Type II diabetes- Women with PCOS have an elevated prevalence of insulin resistance and type II diabetes
- High blood pressure
- Depression / Anxiety
- Dyslipidemia- Disorders of lipid metabolism — cholesterol and triglycerides. PCOS patients show decreased removal of atherosclerosis, inducing remnant
- Cardiovascular disease
- Strokes
- Weight **weight causes PCOS. PCOS causes further weight gain
- Miscarriage
- Acanthosis nigricans- Patches of darkened skin under the arms, in the groin area, on the back of the neck
- Autoimmune thyroiditis- Autoimmune disorders: Hashimoto's thyroiditis and Postpartum thyroiditis
Treatment / Management:
To break free from the vicious cycle of PCOS, first and fore-most one must be willing to accept the fact that PCOS is just another disorder. Simply because it happens to afflict the female reproductive organ, it does NOT assume astronomical damages on your identity or take away from your right to live a life of dignity. In this age, although optimal treatments have not yet been designed for the lack of large scale and reliable clinical trials, several treatments are still offered, specifically tailored to meet the patient’s unique combination of PCOS symptoms.
Some of them are:
1. Lowering circulating Insulin levels by improving Insulin sensitivity through medications such as metformin, and the newer thiazolidinedione (glitazones)
 |
Metformin & Thiazolidinedione |

2. Restoration of fertility: It’s a myth that once PCOS afflicts, a woman cannot conceive. Truth is with proper treatment and subsequent maintenance by imbibing healthy lifestyle changes, any once a PCOS-ed woman can mother.
**There are many success stories.
Please consult your gynecologist for relevant information.
Varied ranges of treatments are available to aid successful conception. Generally intercourse / insemination are advised around ovulation, which is usually predicted by urine tests that detect the preovulatory LH surge (OPKs - ovulation predictor kits). Since OPKs are not very accurate in women with PCOS, charting cervical mucus or fertility monitors that detect changes in urinary hormones and saliva may be employed. Basal body temperatures may also be monitored to confirm ovulation. Ovulation may also be confirmed by testing for serum progesterone at mid-luteal phase, approximately seven days after ovulation (cycle day 21).
Overweight women with PCOS, who are anovulatory, may resort to a clomiphene citrate, FSH or metformin treatments along with healthy diet and exercise routines.
 |
Clomiphene citrate |
In adverse cases, where patients do not respond to clomiphene treatments in combination with diet and lifestyle modification, there are several options available including Assisted reproductive technology (ART - controlled ovarian hyperstimulation with FSH injections), in vitro fertilisation (IVF) and in vitro maturation (IVM – extracting oocytes from unstimulated cycles and matured in vitro).
**A cautionary note: ovarian stimulation with FSH followed by hCG has an associated risk of ovarian hyperstimulation syndrome.
 |
Ovarian drilling |
Alternatively laparoscopic procedures called ‘ovarian drilling’ (puncture of 4-10 small follicles with electrocautery) may be carried out, which often results in either resumption of spontaneous ovulations or ovulations after adjuvant treatment with clomiphene or FSH.
 |
Hirsutism progression |
3. Treatment of hirsutism & acne:
A standard contraceptive pill usually containing cyproterone acetate is effective in reducing the effects of hirsutism. Cyproterone acetate is a progestogen with anti-androgen effects that blocks the action of male hormones that contribute to acne and growth of unwanted facial and body hair. Other drugs with anti-androgen effects include flutamide and spironolactone. Metformin can also reduce hirsutism, perhaps by reducing insulin resistance. Eflornithine (Vaniqa), a topical cream drug acts directly on the hair follicles to inhibit hair growth. Individuals may choose alternatives such as electrolysis or laser treatments, which are both faster and efficient than medical therapies.
 |
Eflornithin - Futamide - Spiranolactone (Aldactone) |
4. Restoration of regular menstruation and prevention of endometrial hyperplasia and endometrial cancer: If fertility is not the primary aim, then menstruation can usually be regulated with contraceptive pills. The purpose of regulating menstruation is essentially for the woman's convenience and overall well-being. There is NO medical requirement for regular periods, so long as they occur sufficiently often (atleast once in 3 months to ensure endometrium – womb lining, is shed enough to prevent risks of cancer).
Most brands of contraceptive pill result in a progesterone withdrawal mimicking natural late luteal phase and inducing menses. Common contraceptive pill containing cyproterone acetate are effective both in restoring menstruation and alleviating hirsutism. Oral progestogen pills may be taken at intervals of 3 months to induce predictable menstrual bleeding. D-chiro-inositol (DCI), a naturally occurring human metabolite may also be taken as a dietary supplement to aid in insulin metabolism.
 |
Cyproterone acetate & D-chiro-Inositol |
Alternatively a uterine progestogen device such as the intrauterine system (Mirena) or the progestin (Implanon) implants may be used to provide simultaneous contraception and endometrial protection, for years.
 |
Mirena- Intra Uterine Device (IUD) & Implanon |

Routine exercise particularly pelvic exercises provide general interventions to reducing weight and insulin resistance (by increasing metabolism) thus reducing hormonal imbalances, restoring ovulation and fertility, alleviating acne and hirsutism. Low-carbohydrate diets help maintain weight loss, along with routine exercise. Some experts recommend a low GI (Glycemic index) diet in which a significant part of total carbohydrates are obtained from fruits, vegetables and whole grain sources.
The key to successful treatment and recovery from PCOS is maintaining the HOPE that, YES, it is possible. The availability of knowledge and effective solutions are widespread and within reach than ever before. Your commitment to a healthy lifestyle is of at most significance in ridding PCOS, just like it is for any other ailment. So one should be open and acceptive of their condition, should reach out and learn as much as possible and put in sincere efforts towards healthier changes in lifestyle.
Again, it cannot be more aptly stressed that:
**Your health- the key to your happiness and those close to you, is your responsibility.
So Cheers!! to Life… without the limits of PCOS.

A few relevant resources:
- http://www.pcosupport.org/
- http://www.pcoshelp.org/
- http://www.ovarian-cysts-pcos.com/
- http://www.medicinenet.com/polycystic_ovary/article.htm
- http://women.webmd.com/tc/polycystic-ovary-syndrome-pcos-topic-overview
I applaud your effort in researching all this and putting it in one place. and as always, simple yet effective language. a good read but a very informative piece.. keep it coming..
ReplyDeletethankyou thankyou :D :)
ReplyDeleteHow i got a cure for PCOS (polycystic ovary syndrome).
ReplyDeleteI actually promised myself that i will do this because i never in life thought i would be cured of PCOS because my gynecologist told me there was no cure and because of this i could not take in and get pregnant. I had PCOS (polycystic ovary syndrome) for 7 years and this was a big pain to me and my husband due to the downcast we felt for not having a child. I experienced irregular periods or no periods at all sometimes, heavy periods, i gained weight (fat). I seeked a cure from one doctor to the other used androgen, clomiphene, metformin and even traveled to different states to see other doctors to no avail. My husband got to know about Dr. ALeta via a testimony he read on the internet on how a woman got a cure and he contacted her with the contact she left. I got the herbal medication and used it for the speculated 3 months that was all i have a son who is just 8 months old. Do not give up just contact her on (aletedwin@gmail.com) on how to get the herbal medication. Thanks and i wish you get cured soon too.
ALL THANKS TO DR WILLIAMS WITH HIS HERB MY WIFE WAS COMPLETELY CURED FROM FIBROID.
ReplyDeleteIs my pleasure to comment on this site and i thank the admin of this site for his/her great work so far.one of the happiest moment in life is when you see your own wife put to bed.this awesome moments makes you a man, I really don't know how to thank DR WILLIAMS for helping my wife get cured for over how many year of suffering from FIBROID. i came across DR Williams contact through a headline news on internet about how DR Williams help a woman to get cured of his fibroid and so many other with PCOS and similar body problem ,i contacted him and he told me how to get his herb,few day later he sent me the herbal portion which my wife take every morning for 21 days, and his medicine was able to shrike the fibroid naturally,and now my wife is 4months old pregnant for our second child, and now she very okay without any side effects whatsoever, If you have fibroid, you can contact him on his email address drwilliams098675@gmail.com for advice and for his product.